
+918929672099
Call UsPeptic Ulcer Disease Explained: Key Symptoms, Causes & Treatment
Dr. Vrundali Kannoth|5 min read|
The burning pain in your stomach that won't go away. The discomfort that wakes you at night or appears when you're hungry. You might wonder if it's just stress or something more serious.
Peptic ulcer disease affects millions of people in India each year. Understanding what is peptic ulcer disease helps you recognise symptoms and seek appropriate treatment before complications develop.
You're not imagining the pain, and you're not alone. This common condition is highly treatable once properly diagnosed. Let's explore what causes these painful sores and how you can find relief.
What is peptic ulcer disease?
Peptic ulcer disease definition describes open sores developing in the lining of your stomach, upper small intestine ("duodenum"), or lower oesophagus. These painful ulcers form when digestive acids damage the protective mucus layer.
Your digestive tract produces strong acid, helping break down food. Normally, a thick mucus layer protects the stomach and intestinal walls from this acid. When this protective barrier breaks down, acid erodes the lining, creating painful ulcers.
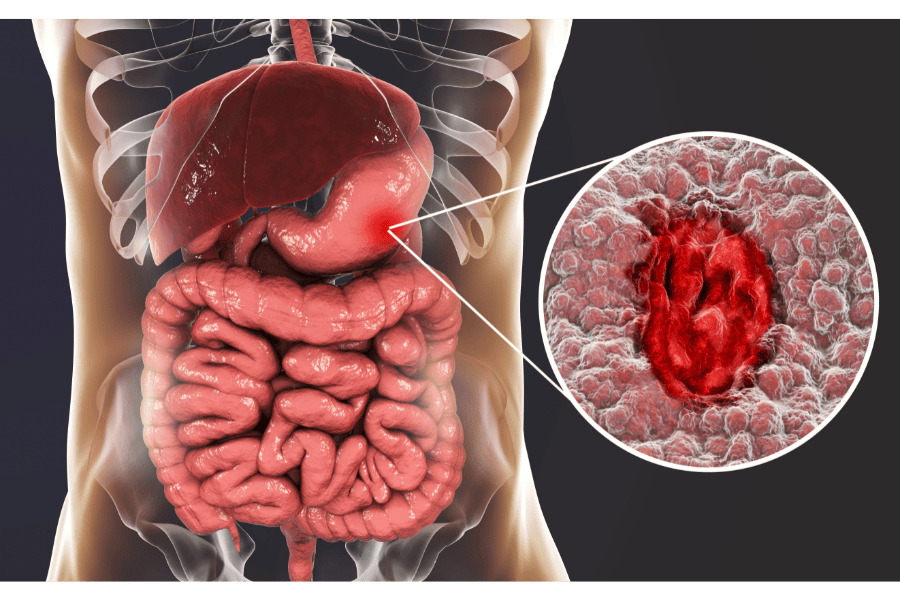
The term "peptic" refers to pepsin, a digestive enzyme working alongside stomach acid. These ulcers can range from a few millimetres to several centimetres in diameter.
According to research, peptic ulcer disease affects approximately 10-15% of Indians at some point during their lives. Whilst common, many cases go undiagnosed because symptoms are mistaken for simple indigestion.
Types of peptic ulcer disease
Types of peptic ulcer disease are classified by location in the digestive tract.
- •Gastric ulcersStomach ulcers develop in the stomach lining itself. Pain typically worsens with eating as stomach acid production increases. These ulcers are more common in older adults and carry a slightly higher cancer risk.
- •Duodenal ulcersThese form in the duodenum, the first part of your small intestine just beyond the stomach. They're more common than gastric ulcers, representing about 80% of cases. Pain often improves with eating but returns 2-3 hours later when the stomach empties.
- •Oesophageal ulcersRare ulcers developing in the lower oesophagus, usually associated with severe acid reflux. They cause difficulty swallowing and chest pain.
Symptoms and causes of peptic ulcer disease
Understanding peptic ulcer disease symptoms and what causes peptic ulcer disease helps you recognise when to seek medical attention.

Common symptoms of peptic ulcer disease
Signs of peptic ulcer disease vary in intensity but typically include characteristic patterns.
Persistent upper abdominal pain:
Peptic ulcer disease pain is the hallmark symptom. It's typically burning or gnawing, located in the upper central abdomen between your breastbone and navel. Pain intensity ranges from mild discomfort to severe distress.
Duodenal ulcer pain often awakens you at night when your stomach is empty. Eating temporarily relieves it. Gastric ulcer pain may worsen with meals.
Indigestion or bloating:
Persistent indigestion with fullness, belching, or bloating accompanies many ulcers. You might feel uncomfortably full after eating small amounts.
Nausea and vomiting:
Frequent nausea occurs, sometimes with vomiting. Severe ulcers may cause vomiting blood (appearing bright red or like coffee grounds).
Appetite loss or weight changes:
Fear of eating because it triggers pain leads to appetite loss and weight reduction. Conversely, some people eat more frequently because food temporarily relieves duodenal ulcer pain.
Other warning signs:
- •Dark, tarry stoolsindicating bleeding
- •Unexplained fatiguefrom chronic blood loss
- •Pale skinfrom anaemia
Many people ignore early symptoms, attributing them to stress or dietary indiscretions. This delay worsens the peptic ulcer disease condition and increases complication risk.
Causes of peptic ulcer disease
Two main causes account for most peptic ulcers.
H pylori infection:
This spiral-shaped bacterium burrows into stomach and duodenal mucus layers, weakening protective barriers and allowing acid damage. Approximately 50-60% of Indians carry H. pylori, though most never develop ulcers.
The bacteria spreads through contaminated food, water, or close contact with infected individuals. Poor sanitation increases infection rates, explaining higher prevalence in developing regions.
NSAID use:
Non-steroidal anti-inflammatory drugs like aspirin, ibuprofen, and diclofenac damage the stomach lining's protective mechanisms. Regular use significantly increases ulcer risk, particularly in older adults.
Common NSAIDs prescribed in India are diclofenac, aceclofenac, ibuprofen, and all carry this risk. Taking these medications with food doesn't prevent ulcers.
Less common causes:
- •Zollinger-Ellison syndrome(rare condition causing excessive acid production)
- •Severe physiological stress(major surgery, burns, critical illness)
- •Certain cancers
- •Chronic diseasesaffecting mucus production
Importantly, spicy food and stress don't directly cause ulcers, though they may worsen existing ones.
Risk factors for peptic ulcer disease
Risk factors for peptic ulcer disease help identify who's most vulnerable.
Major risk factors include:
- •H. pylori infection
- •Regular NSAID use
- •Smoking(delays healing and increases recurrence)
- •Excessive alcohol consumption
- •Age over 50
- •Family history of ulcers
- •Concurrent use of corticosteroids
- •Previous ulcer history
Complications of peptic ulcer disease
Complications of peptic ulcer disease can be serious, requiring emergency treatment.
- •Internal bleedingUlcers can erode blood vessels, causing slow bleeding (leading to anaemia) or severe haemorrhage requiring transfusion. This is the most common serious complication.
- •PerforationDeep ulcers can create holes through stomach or duodenal walls, spilling digestive contents into the abdominal cavity. This causes severe pain and requires emergency surgery.
- •ObstructionScarring from chronic ulcers can narrow the digestive tract, blocking food passage. Symptoms include severe bloating, vomiting, and weight loss.
- •Cancer riskCan stomach ulcers cause cancer ? Chronic gastric ulcers, particularly those related to H. pylori infection, slightly increase stomach cancer risk. This is why persistent ulcers need careful monitoring.
Diagnosis and medical evaluation
Peptic ulcer disease diagnosis involves several approaches confirming ulcers and identifying underlying causes.
Medical history and physical examination:
Your doctor asks about symptoms, NSAID use, and medical history. Physical examination assesses abdominal tenderness and checks for complications.
Upper endoscopy:
This peptic ulcer disease medical procedure is the gold standard diagnostic test. A thin, flexible tube with a camera passes through your mouth into your stomach and duodenum.
Doctors directly visualise ulcers, assess size and location, and take tissue samples (biopsies). Does endoscopy detect cancer ? Yes, biopsies identify malignant changes requiring different treatment approaches.
Most major hospitals across India offer endoscopy services. The procedure takes 15-30 minutes under sedation, causing minimal discomfort.
H. pylori testing:
Several tests detect H. pylori infection:
- •Stool antigen test
- •Breath test (urea breath test)
- •Blood antibody test
- •Biopsy during endoscopy
Imaging studies:
X-rays with barium contrast can reveal ulcers, though endoscopy provides more detailed information. CT scans identify complications like perforation.
Treatment and management of peptic ulcer disease
Peptic ulcer disease treatment focuses on healing ulcers, eliminating H. pylori if present, and preventing recurrence.
Peptic ulcer disease medications:
- •Proton pump inhibitors (PPIs)These powerful acid suppressants are primary peptic ulcer disease drugs. They promote healing by reducing acid production dramatically.
- •H2 receptor blockersRanitidine (now withdrawn), famotidine, and cimetidine reduce acid production less powerfully than PPIs. They're sometimes used for mild cases or maintenance therapy.
- •AntibioticsH. pylori eradication requires combination antibiotic therapy.
- •AntacidsOver-the-counter antacids provide temporary symptom relief but don't heal ulcers.
- •Protective agentsSucralfate coats ulcers, protecting them from acid. Misoprostol prevents NSAID-induced ulcers in high-risk patients requiring continued NSAID use.
Protective agents:
Sucralfate coats ulcers, protecting them from acid. Misoprostol prevents NSAID-induced ulcers in high-risk patients requiring continued NSAID use.
Lifestyle modifications:
Sucralfate coats ulcers, protecting them from acid. Misoprostol prevents NSAID-induced ulcers in high-risk patients requiring continued NSAID use.
- •Stop smoking(significantly improves healing)
- •Limit alcohol consumption
- •Avoid NSAIDswhen possible; discuss alternatives with your doctor
- •Manage stressthrough relaxation techniques
- •Eat regular, balanced meals
Surgical intervention:
Surgery is rarely needed today thanks to effective medications. Indications include:
- •Perforationrequiring emergency repair
- •Severe bleedingnot controlled by endoscopic techniques
- •Obstructionfrom scarring
Procedures include gastrojejunostomy (creating bypass around obstruction), vagotomy (cutting nerves stimulating acid production), or partial gastrectomy (removing part of stomach).
Proper management of peptic ulcer disease achieves healing rates exceeding 90% within 4-8 weeks.
Key takeaways
Peptic ulcer disease creates painful sores in your stomach or duodenal lining, primarily caused by H. pylori infection or regular NSAID use.
Modern peptic ulcer disease cure approaches achieve excellent healing rates with appropriate medication combinations, typically PPIs with antibiotics if H. pylori is present.
Prevention of peptic ulcer disease focuses on avoiding NSAIDs when possible, treating H. pylori infections promptly, and eliminating smoking.
Don't ignore persistent abdominal pain or indigestion. Early diagnosis and treatment prevent serious complications of peptic ulcer disease like bleeding or perforation. Peptic ulcer disease statistics show that while common, this condition responds well to treatment when addressed promptly.
Connect with experienced gastroenterologists and oncology doctors who can provide accurate diagnosis, appropriate cancer treatment if malignancy is discovered, and comprehensive prognosis of peptic ulcer disease, tailored to your specific needs.
FAQs
Common questions about this topic
Most peptic ulcers heal within 4-8 weeks with proper medication. H. pylori-related ulcers require antibiotic completion before healing begins. NSAID-induced ulcers heal faster once NSAIDs are stopped.
Related Blogs
Symptoms5 min read
Recognising the Signs of Cancer in the body that often go unnoticed
Dr. Vrundali Kannoth

Prevention5 min read
Is Cervical Cancer Caused by an STI? Understanding the HPV Connection
Dr. Vrundali Kannoth