Symptoms5 min read
Folic Acid Supplement: Importance, Benefits and Deficiency Symptoms
Dr. Vrundali Kannoth
Learning that you have a mediastinal tumour can feel overwhelming. Because it develops near vital organs like the heart and lungs, it’s natural to feel scared or uncertain while trying to make sense of unfamiliar medical terms.
If you’re feeling anxious, know that many mediastinal tumours are benign (non-cancerous), and most can be effectively managed with modern medical care.
In fact, mediastinal tumours are usually discovered accidentally during a routine scan, and most people live perfectly normal lives after mediastinal tumour treatment.
This guide describes what a mediastinal tumour is, explains the types, and shows you the clear, advanced path toward healing.
To understand the tumour, it’s critical to first understand the mediastinum. It is the space in the middle of your chest that holds multiple critical internal organs and mainly connects the two lungs.
A mediastinal tumour is simply an abnormal growth of cells that starts in this central space.
Because this area is so crowded, even a small mediastinal tumour can sometimes lean on a nerve or a blood vessel, which is often how they get noticed.
The mediastinum is divided into three compartments. Knowing which compartment the tumour is in tells your oncologists exactly what kind of growth they are likely dealing with.
| Mediastinal compartment | Location | Description |
|---|---|---|
| Prevascular (anterior) compartment | Front of the chest, behind the breastbone (sternum) | The anterior part of the mediastinum is located between the sternum and the heart structures |
| Visceral (middle) compartment | Central area of the chest | Contains the heart, major blood vessels, trachea, and main airways |
| Paravertebral (posterior) compartment | Back of the chest, near the spine | Located alongside the vertebral column; contains structures related to nerves and the spine. |
Here are the three compartments discussed in more detail:
This is the most common location for tumours in adults (about 50% of cases). You might find your oncologist referring to the "4 T's" when looking at this area:
The most common middle mediastinal tumours are usually benign, such as pericardial cysts (near the heart). They are usually harmless but might be removed if they grow large enough to cause pressure.
Bronchogenic carcinoma (near the windpipe) can also sometimes extend into the mediastinum. So, it’s necessary to distinguish it from primary mediastinal growths.
In children, this is the most common spot for mediastinal tumours. They usually start in the nerve tissues (neurogenic tumours). Most of these, like Schwannomas, are benign and easily treated, though some in infants can be more aggressive.
Rarely, tumours with similar symptoms may include a neuroendocrine tumour.
Although modern imaging focuses on three compartments, some older anatomical descriptions still refer to superior mediastinal tumours, which overlap mainly with anterior and middle compartment masses.
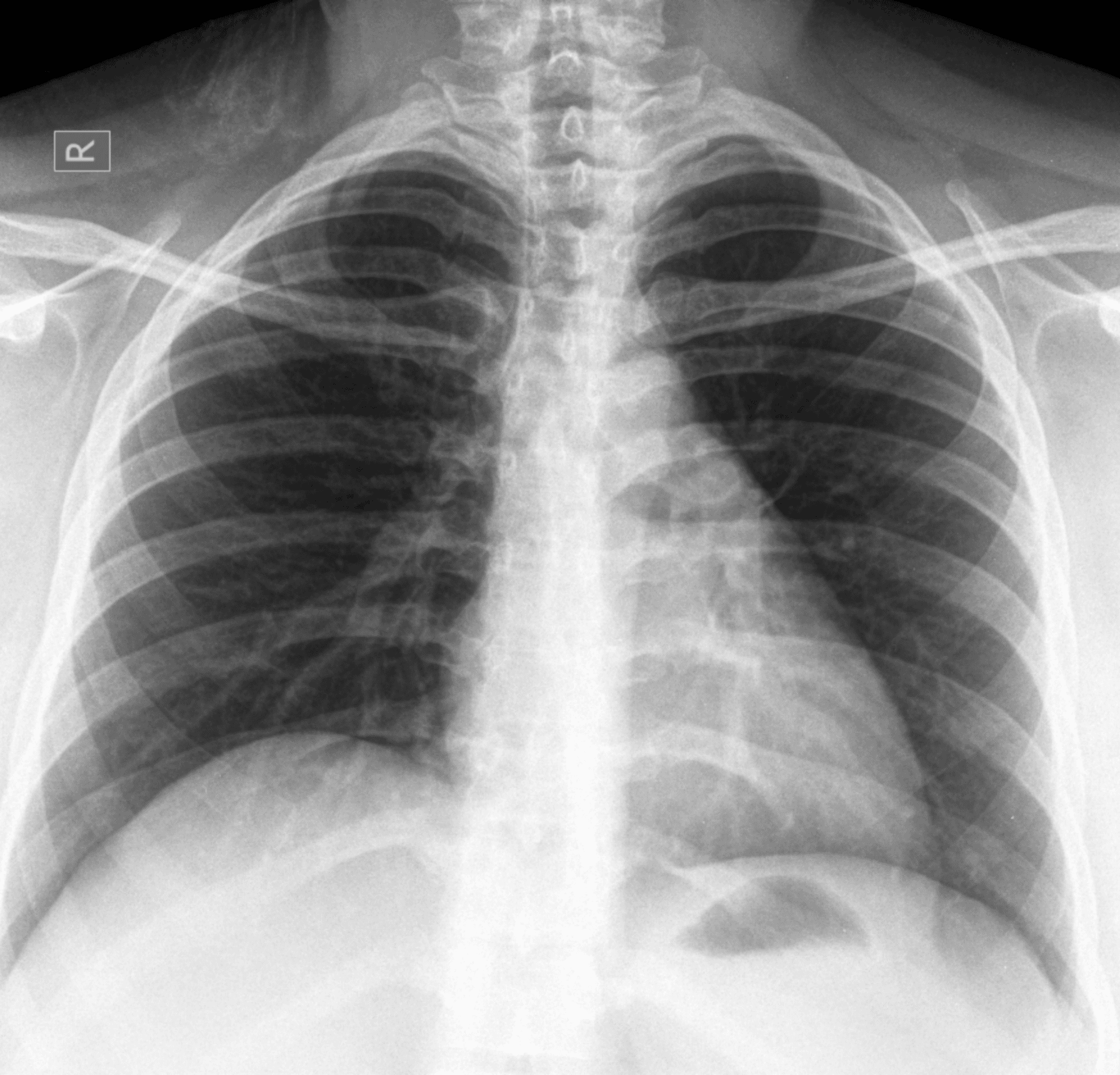
Roughly 40% of people have no symptoms of mediastinal tumours at all. Your tumour was likely found when you got a chest X-ray for a persistent cough or a minor injury. However, because the chest is a tight space, symptoms can occur when a mediastinal tumour starts "pushing" on other internal organs.
The symptoms originating from the pressure are:
Some tumours are "biologically active." For example, 30–50% of people with a thymoma develop Myasthenia Gravis, a condition that causes muscle weakness, often starting in the eyes or face.
Despite common beliefs and unlike lung cancer, mediastinal tumours aren't usually linked to smoking. They often stem from:
If your pathologist suspects a tumour, they may use non-invasive imaging techniques first to diagnose the tumour growth:
| Imaging test | What it does | What pathologists learn |
|---|---|---|
| CT scan | Detailed cross-sectional chest images | Shows tumour size, exact location, and whether it touches blood vessels or airways; can detect fat or calcification |
| MRI | High-detail soft tissue imaging | Helps evaluate posterior tumours and tells solid tissue apart from fluid-filled cysts. Chemical-shift MRI is particularly useful for differentiating thymic hyperplasia from a malignant neoplasm. |
| PET scan (PET-CT) | Measures cell activity using a small amount of radioactive sugar | Helps distinguish benign growths from aggressive cancers and is important for lymphoma staging |
Imaging also helps distinguish superior mediastinal tumours from masses arising lower in the chest.
If your tests are still not conclusive about benign and malignant tumours, you might be asked to undergo a biopsy. The type of biopsy you’re gonna get will depend on the location and type of your mediastinal tumour. Some of the more invasive procedures to confirm the diagnosis are:
Mediastinal tumour staging is used to describe the stages of cancer. This helps oncologists to know how fast your mediastinal tumour is growing.
For many years, pathologists used the Masaoka-Koga system, which looked at whether the tumour had broken through its "capsule" (like the skin of a grape). The technology has now moved toward the TNM system, which is more precise.
The 9th Edition update even looks at tumour size. If a tumour is under 5 cm, it's categorised differently from one over 5 cm. This allows oncologists to be much more specific with their treatment plans rather than using a one-size-fits-all approach.
Here is a quick overview of what the tumour stagings mean:
| Stage | What it means |
|---|---|
| Stage I | The tumour is contained within its "shell" or the nearby fat. Highly treatable. |
| Stage II/III | The tumour has started to grow into nearby organs (like the heart lining). |
| Stage IV | The tumour has spread to more distant parts of the chest or other organs. |
The goal of mediastinal tumour treatment is always to remove or shrink the growth while protecting your vital organs.
The surgeries have moved from sternotomy (opening the breastbone) to VATS and robotic surgery.
Most mediastinal tumour surgery procedures now use tiny incisions and robotic arms (like the Da Vinci system) to remove tumours. This means less pain, smaller scars, and a much faster recovery.
For more aggressive tumours, oncologists no longer just rely on standard chemotherapy. Immunotherapy helps your own immune system find and eliminate the cancer cells. This has been helpful for cases that were once considered difficult to treat.
Precise beams of energy can be used to clean up any microscopic cells left behind after surgery, ensuring the tumour doesn't come back.
A mediastinal tumour diagnosis can feel frightening. But it is important to remember that most of these growths are benign, and malignant tumours are highly treatable. The mediastinal tumour survival rate is also excellent when diagnosed early. Modern imaging, precise staging, and minimally invasive treatments allow oncologists to plan care safely and effectively.
With early evaluation and the right cancer treatment approach, most patients recover well and return to their normal routines. You are not expected to navigate this journey alone.
Clear guidance, experienced care, and compassionate support can make each step more manageable, helping you move forward with confidence, reassurance, and hope.